
Aatrix Complete ACA eFiling
Supported Forms
Is Aatrix supporting the ACA reporting?
Yes, Aatrix will be supporting the 6055 & 6056 reporting requirements. The information will be reported on the 1095/94-B or the 1095/94-C form sets.
FORM 1095-C
Click on the individual boxes below for specific IRS Instructions
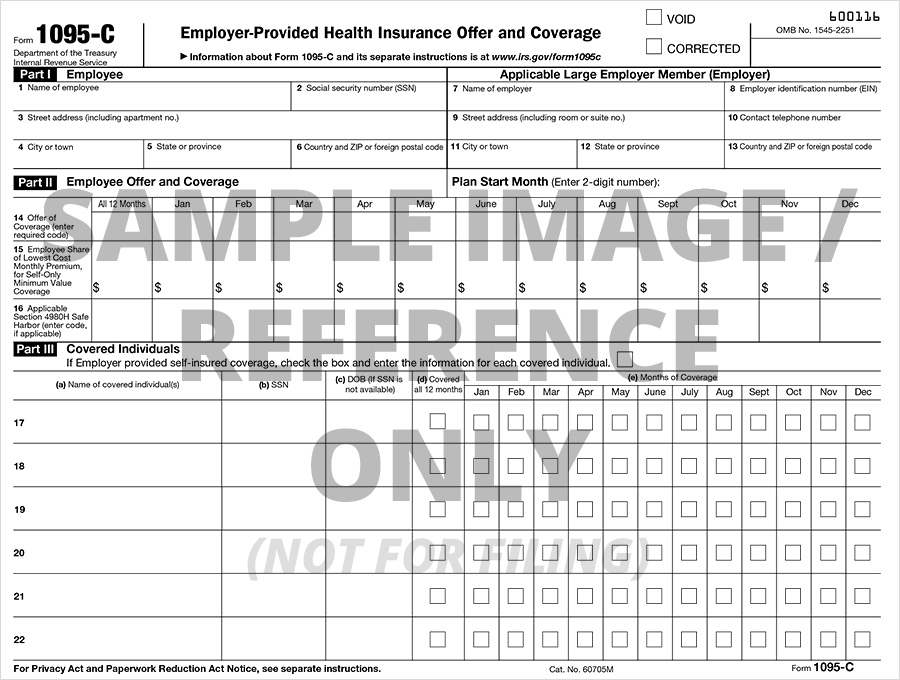
| Part I: Employee Applicable Large Employer Member (ALE Member/Employer) | |||||||||
|
| Part III: Covered Individuals |
| Part III Lines 17-22, Covered Individuals |
FORM 1094-C
Click on the individual boxes below for specific IRS Instructions
| Part II: ALE Member Information |
| Line 20, Total Number of Forms filed by and/or on behalf of the employer. |
| Line 21, ALE Member is part of Aggregated ALE Group |
| Line 22, Certifications of Eligibility |
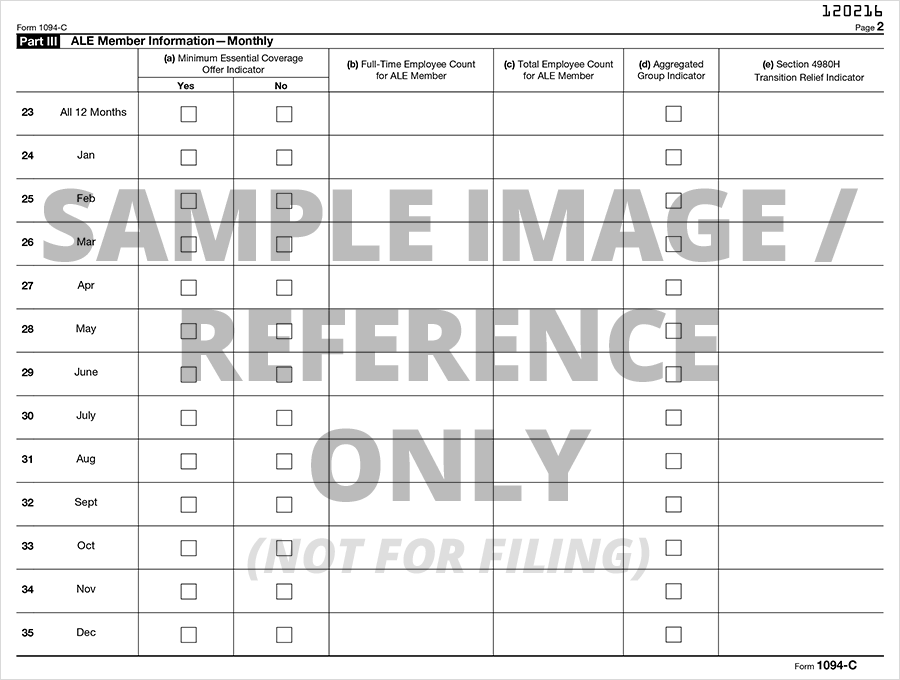
| Part III: ALE Member Information — Monthly (Lines 23–35) |
| Column (a), Minimum Essential Coverage |
| Column (b), Full-Time Employee Count for ALE Member |
| Column (c), Total Employee Count for ALE Member |
| Column (d), Aggregated Group Indicator |
| Column (e), Aggregated Group Indicator |
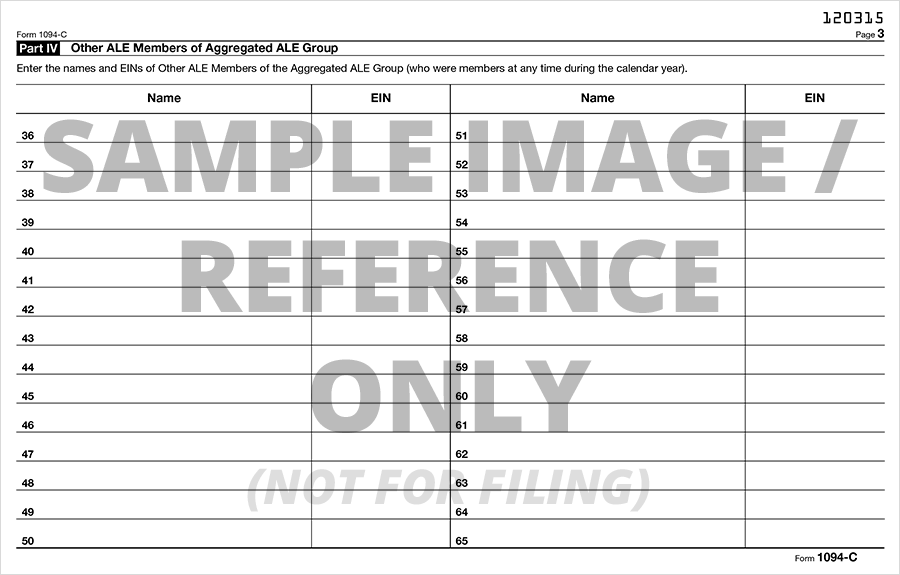
| Part IV: Other ALE Members of Aggregated ALE Group |
| Lines 36-65, Other ALE Members of Aggregated ALE Group |
FORM 1095-B
Click on the individual boxes below for specific IRS Instructions
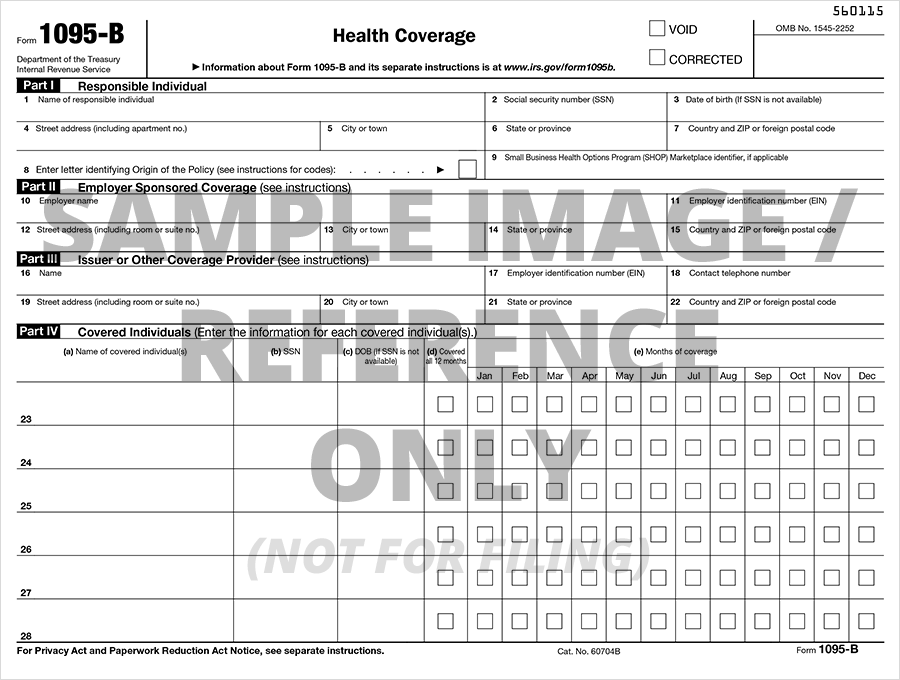
| Part I: Responsible Individual |
| Part II: Employer-Sponsored Coverage |
| Lines 10-15, Name, EIN, and Complete Mailing Address for the Employer Sponsoring the Coverage |
| Part III: Issuer or Other Coverage Provider |
| Lines 16-22, Name, EIN, and Complete Mailing Address of Issuer/ Other Coverage |
| Part IV: Covered Individuals |
| Column (a), Covered Individual's Name |
| Column (b), Covered Individual's Social Security Number (SSN) |
| Column (c), Covered Individual's Birthdate (MM/DD/YYY) if Social Security Number (SSN) is not available |
| Column (d), Covered all 12 months |
| Column (e), Months of Coverage |
| Part IV: Covered Individuals (Continuation) |
| Column (a), Name of each Covered Individual |
| Column (b), Social Security Number (SSN) of each Covered Individual |
| Column (c), Birthdate (MM/DD/YYY) of each Covered Individual if SSN is not available |
| Column (d), Individual Covered for 12 months |
| Column (e), Coverage each month if individual wasn't covered for all 12 months |
FORM 1094-B
Click on the individual boxes below for specific IRS Instructions
| Part IV: Covered Individuals (Continuation) |
| Line 1, Filer's Complete Name |
| Line 2, Filer's EIN |
| Lines 3 and 4, Contact Person's Name and Telephone Number |
| Lines 5-8, Filer's Complete Address |
| Line 9, Total number of 1095-B forms transmitted with 1094-B |